Research article / Open Access
DOI: 10.31488/bjcr.216
Biophysical Skin Parameters and Skin Related Quality of Life in Breast Cancer Patients
Monica Iorfida1, Paola Perugini2, 3, Maria Vittoria Visconti4, 5, Matilde Monteleone4, Camilla Ottomano4, 5, Giulio Tosti6, Damaris Patricia Rojas7, 8, Patrick Maisonneuve9, Emanuela Omodeo Sale’4, 10
1.Division of Medical Senology, European Institute of Oncology, IRCCS, Milan, Italy
2.Department of Drug Sciences, University of Pavia, Italy
3.Etichub s.r.l., Academic spin off, Via Taramelli 12, 27100 Pavia
4.Division of Pharmacy, European Institute of Oncology, IRCCS, Milan, Italy
5.Department of Pharmaceutical Sciences, University of Milan, Milan, Italy
6.Dermato-Oncology Unit, European Institute of Oncology IRCCS, 20141 Milan, Italy
7.Department of Radiation Oncology, European Institute of Oncology, 20141 Milan, Italy
8.Department of Oncology and Hemato-Oncology, University of Milan, 20122 Milan, Italy
9.Division of Epidemiology and Biostatistics, European Institute of Oncology IRCCS, Milan, Italy
10.Centro Cardiologico Monzino IRCCS, 20138 Milano, Italy
*Corresponding author:Paola Perugini, Department of Drug Sciences, University of Pavia, Etichub s.r.l., Academ- ic spin off, Via Taramelli 12, 27100 Pavia, E-mail: paola.perugini@unipv.it
Abstract
Background Breast cancer is the most frequently diagnosed cancer among women worldwide. Aromatase inhibitors (AIs) and taxane-based chemotherapy are key treatments both associated with dermatologic adverse events (dAEs) that impair skin physiology and patient-reported outcomes. Patients and Methods This cross-sectional study included 81 female breast cancer patients treated with aromatase inhibitors or taxanes. Skin assessments covered barrier function, hydration, transepidermal water loss (TEWL), roughness, pigmentation, thickness, collagen, and elasticity by using bioengineering techniques. Quality of life (QoL) was evaluated by Skindex-29. Analyses accounted for age, treatment type, and time since surgery. Results Assessment of skin barrier integrity revealed that TEWL values varied according to time since surgery rather than treatment type. A similar trend was observed for skin redness, whereas instrumental measurements of skin texture (Ra) showed a distinct age-dependent pattern regardless of pharmacological therapy. Skindex-29 revealed that 20% of patients on aromatase inhibitors and 23% on taxane-based chemotherapy reported physical symptoms, while 9% and 11%, respectively, reported emotional distress related to these symptoms. Conclusions Time from surgery and age primarily influence objective skin parameters in breast cancer survivors. Integrating instrumental measures with patient-reported outcomes identifies key targets for personalized skincare in supportive oncology care, potentially enhancing QoL.
Keywords: breast cancer, dermatologic toxicity, Skindex-29, adjuvant therapy
Introduction
With approximately 2.3 million new cases identified, breast cancer represented the most common cancer diagnosis globally, thus highlighting its significant impact on the global healthcare system. [1,2].
Aromatase inhibitors (Ais; anastrozole, letrozole, exemestane) therapy is a well-established treatment for estrogen receptor-positive (ER+) breast cancer, which constitutes over 70% of all cases. AIs act by inhibiting aromatase, an enzyme that converts androgens to estrogens in peripheral tissues, thereby reducing estrogen levels and limiting cancer progression [3].
Adjuvant endocrine therapy with aromatase inhibitors (AIs) is standard for postmenopausal women with estrogen receptor-positive (ER+) disease (>70% of cases), offering superior disease-free survival versus tamoxifen [4].
Although the clinical benefit of AIs is well established, their safety profile warrants careful consideration, particularly regarding under-recognized toxicities. While musculoskeletal and bone-related side effects have been extensively documented, dermatologic adverse events (dAEs) are less commonly reported despite their potential to impair quality of life and treatment adherence. Recent evidence from a pharmacovigilance analysis of the FDA Adverse Event Reporting System (FAERS) identified 2,237 AI-related dermatologic cases among more than 21 million reports [5].
The analysis revealed 61 preferred terms with positive signals, including nail disorders, onychoclasis, and abnormal hair growth. The strongest associations were observed for pseudo-cellulitis (reporting odds ratio [ROR] 57.73), anhidrosis (ROR 48.68), and nail toxicity (ROR 38.40). Notably, significant correlations were found for anastrozole (ROR 1.07, 95% CI 1.03–1.11) and exemestane (ROR 1.10, 95% CI 1.04–1.16), whereas letrozole did not demonstrate a statistically significant association. Latency analysis showed that certain dermatologic events could appear as early as two days after AIs initiation, while others, such as skin ulceration with exemestane, emerged after more than 200 days of treatment.
The enzyme aromatase is expressed in several tissues, including ovarian granulosa cells, adipose and skin fibroblasts, bone, and the brain. In postmenopausal women, peripheral aromatization, particularly in adipose tissue and skin, becomes the primary source of estrogen and increases with age and body weight. [6] Estrogen biosynthesis in the skin occurs in keratinocytes, melanocytes, and fibroblasts, and plays a vital role in skin physiology. Estrogen promotes the expression of structural proteins including ezrin, hyaluronic acid (which contributes to skin hydration and thickness), elastin (resilience), and collagen (dermal mass) [7]. Consequently, the profound estrogen depletion caused by AIs therapy can lead to skin dryness, thinning, atrophy, delayed wound healing, increased irritation, and pruritus highlighting the need for a monitoring system to detect and promptly manage skin toxicities.
Taxane-based chemotherapy is a cornerstone in both early and metastatic settings, reducing recurrence when added to anthracyclines [8-10].
Taxanes are implicated in cutaneous reactions in approximately 65% of patients, including alopecia, hypersensitivity reactions, nail disorders, and morbilliform rashes [11,12]. Severe delayed reactions - such as radiation recall dermatitis, palmar-plantar erythrodysesthesia, Stevens–Johnson syndrome, acute generalized exanthematous pustulosis, and autoimmune skin diseases like systemic lupus erythematosus and subacute cutaneous lupus erythematosus - though rare, may also occur [13,14].
Despite efficacy, both therapies carry dermatologic adverse events (dAEs) impacting quality of life (QoL) and adherence [15,16].
Few studies quantify dAEs via objective biophysical parameters (transepidermal water loss [TEWL], hydration, elasticity, color, texture [Ra]). This cross-sectional study evaluates skin integrity, physiology, and Skindex-29-reported QoL in 81 breast cancer survivors stratified by age, time since surgery, and treatment (taxane- vs AI-based) [17]. Findings aim to identify therapy-independent patterns and support personalized toxicity management.
Patients and Methods
Study design and participants
The study adopted a cross-sectional design. Convenience sampling identified 89 eligible women (aged 40–70 years) post-surgery for breast cancer receiving adjuvant aromatase inhibitors (AI; anastrozole/letrozole/exemestane), paclitaxel (±radiotherapy), or tamoxifen. Tamoxifen patients (n=6) and ineligible cases (n=2) were excluded, yielding 81 patients stratified by age, time since surgery, and therapy (AIs n=61; taxane n=20).
Inclusion criteria:
• Age between 40 and 70 years;
• Active treatment with tamoxifen, aromatase inhibitors, or paclitaxel as adjuvant therapy, with or without radiotherapy;
• Subjects receiving hormonal therapy must have discontinued any chemotherapy at least 30 days prior;
• Acquisition and signing of informed consent and privacy information.
Exclusion criteria:
• Presence of chronic skin diseases known prior to the start of adjuvant treatment (psoriasis, lupus, atopic dermatitis);
• Inability to understand and/or provide informed consent;
• Unwillingness or inability to complete all tests required by the protocol;
The study was approved by the IEO Institutional Review Board (project code: UID 4588/12_March_2024) and conducted in accordance with the principles stated in the Declaration of Helsinki and the guidelines of Good Clinical Practice.
Skindex-29 questionnaire
The Skindex-29 questionnaire is a patient-reported outcome measure designed to assess the impact of dermatological conditions on quality of life (QoL), effectively capturing subjective distress that may be overlooked by conventional clinical instruments such as the Common Terminology Criteria for Adverse Events (CTCAE) [17]. It comprises 29 items divided into three domains: symptoms (7 items – numbers 1, 7, 10, 16, 19, 24, 27), emotional functioning (11 items – numbers 3, 6, 9, 12, 13, 15,18, 21, 23, 26, 28), and social functioning (12 items – numbers 2, 4, 5, 8, 11, 14, 17, 20, 22, 25, 29). Each item evaluates the frequency of skin-related issues experienced by patients over the preceding four weeks a timeframe chosen for its clinical relevance, as it generally allows patients to attain a new homeostatic state following changes in dermatologic treatment.
The questionnaire is self-administered and validated in international literature, with responses based on a five-point Likert scale: “never,” “rarely,” “sometimes,” “often,” and “all the time,” corresponding to scores of 0, 25, 50, 75, and 100, respectively. Higher scores indicate a greater impact of the skin condition on Quality of life. They can be classified according to established domain-specific cut-off values as absent, mild, moderate, or severe [18, 19]. During analysis of the Skindex-29 items, the questions were grouped into the three macro-categories identified in the questionnaire's original structure. This allowed for a more immediate and coherent interpretation of the data.
These macro-domains reflect the principal areas of impact evaluated by the Skindex-29: physical symptomatology, emotional distress, and interference with daily and social functioning.
For percentage calculations, only scores ranging from 50 to 75 were considered, as they were interpreted as indicative of moderate discomfort.
We supplemented the official Skindex-29 with an initial section collecting patients' demographic and clinical data, thereby enabling a more comprehensive characterization of the population under investigation. The questionnaire was administered on the same day as the cutaneous tests.
Instrumental measurements
The instruments used to evaluate skin parameters involve contact between the upper arm (the test area) and a series of probes that do not cause discomfort, pain, or skin damage.
Skin barrier integrity was assessed by the measurement of transepidermal water loss (TEWL) and the stratum corneum hydration (SCWC). TEWL from 0 to 90 g*m-2h-1 was detected using a skin evaporimeter made of a small cylindrical open chamber (1 cm in diameter, 2 cm in height) with a couple of hygrometric sensors connected to a microprocessor plugged into a computer workstation, using Tewameter TM 300 (Cutometer MPA580, Courage & Khazaka). Stratum corneum hydration was evaluated using a CM 825 corneometer (Cutometer MPA580, Courage & Khazaka). Corneometry is a technique used to assess the hydration of the outermost layer of the epidermis, the stratum corneum [20]. Since skin is a dielectric medium, all variations in hydration result in a corresponding change in the skin's electrical capacity. The device used in the present trial was equipped with a 49 mm2 surface probe that allows precise measurements within 1 second over a depth range of 10–20 μm in the stratum corneum . The parameter was expressed using an arbitrary score scale (0–100 A.U.).
The thickness of the upper layers of the skin (epidermis and dermis) and the collagen intensity were evaluated by ultrasound images obtained by a 22 MHz DUB system (DermaLab Combo Ultrasound Standard probe (Cortex technology, Hadsund, Denmark). The first parameter represents the distance between the epidermis and the dermis/hypodermis boundary, while the second parameter reflects the structural density, indicating the amount and the activity of collagen present in the dermis.
The morphological aspects of the skin, including surface texture, fine-line profile, redness, and pigmentation, were evaluated using dedicated software for three-dimensional images acquired with Antera 3D. (Miravex Limited, Dublin, Ireland). [21] The 3D image acquired with the instrument can be transformed using specific software into a color image in which each shade of color (from blue to yellow) is related to a height; thus, the presence of a groove will be indicated by a color gradient that can transition from blue to green according to its depth. Parameters characterizing skin micro-reliefs which can be measured at a glance, immediately thanks to this 3D topographic representation of the skin are the following:
• Ra represents the average skin roughness texture. It is the integral of the function describing the skin roughness profile curve; the higher the value of Ra, the higher the skin roughness.
• Rt represents the maximal skin roughness. Single roughness depths are first determined by measuring the peak-to-valley distance within each evaluated sampling length. Rt is the greatest peak-to-valley distance within any single sampling length, which is defined as the vertical distance between the top of the highest peak and the bottom of the lowest valley.
The average concentration and uniformity of biochromophores, such as melanin and hemoglobin, in the skin were also investigated to detect pigmentation alterations and redness areas.
Parameters characterizing the pigmentation are the following:
• Minimum: a minimum concentration of pigmentation per unit area relative to the area selected;
• Maximum: a maximum concentration of pigmentation per unit area relative to the area selected;
• Variation: description of the extent of the color or pigmentation differences in the skin giving information of the uniformity of the pigment
Parameters characterizing the redness are the following:
• Minimum: a minimum concentration of hemoglobin per unit area relative to the area selected;
• Maximum: a maximum concentration of hemoglobin per unit area relative to the area selected;
• Variation: description of the extent of the redness differences in the skin giving information of the redness uniformity.
The skin's mechanical properties were measured using an MPA580 cutometer (Courage & Khazaka). [22] In this technique, the skin is evaluated by measuring the vertical deformation induced by vacuum aspiration at a negative pressure of 450 mbar, applied to the skin for 1-3 seconds via a 2 mm probe. The parameters considered were:
R0: Skin firmness. This parameter measures the maximum amplitude, expressed in mm, that the skin reaches after the cutometer applies suction and represents the passive response of the skin to applied force. R0 represents the ratio of skin looseness to skin tightness; the lower R0 is, the firmer the skin.
R2: An index representing the capability of the skin to return to its rest condition after being exposed to mechanical stress, that is, a percentage of the total elasticity of the skin. The closer R2 is to 100, the more elastic the skin is.
R5: The ratio between the skin's immediate recovery and its immediate deformation. Therefore, it is a measure of the net elasticity, expressed as a percentage.
Statistical analysis
We limited the primary analysis to 81 patients who received either aromatase inhibitors or taxanes for the treatment of breast cancer.
For each skin measure, we calculated the average of the left and right arm measurements and analyzed them separately for the affected and unaffected sides.
For the primary study endpoint, we used a one-sample t-test to assess whether the mean hydration of the entire population was significantly greater than a reference value (mean=39.0, standard deviation=6.9) from the general population.
Patient characteristics were presented as frequencies and percentages, and their distributions were compared using Fisher's exact test.
Skin parameters were presented as means ± standard deviations. Comparison across different age groups (0-49, 50-59, 60+), time since surgery (<1, 1-5, >5 years), and current treatment groups (aromatase inhibitors, taxanes) was made using univariable and multivariable generalized linear models mutually adjusted for age, years since surgery, and current treatment group.
We used violin plots to show the distributions of various skin parameters within the same age, time since surgery, and current treatment groups. Paired comparisons of medians were performed using the non-parametric Wilcoxon test, while overall comparison was made using the Kruskal-Wallis test.
All tests were two-sided with α=0.05. Analyses were performed using the SAS software version 9.4 (Cary, NC).
Results
Eighty-one patients satisfied the inclusion and exclusion criteria and were enrolled in the study. At the time of the study, 61 patients were receiving aromatase inhibitors and 20 were receiving taxanes as adjuvant treatment. Patients' characteristics are given in Table 1.
Table 1 Patients’ characteristics
| Characteristic | Total (N=81) | Treatment Type | p-value | |
|---|---|---|---|---|
| Aromatase Inhibitors (N, col %) | Taxanes (N, col %) | |||
| All patients | 81 | 61 (100) | 20 (100) | |
| Age (Median [range]) | 57 [27–82] | 60 [39–82] | 48 [27–70] | |
| 0–49 | 17 | 6 (9.8) | 11 (55.0) | <0.0001 |
| 50–59 | 28 | 23 (37.7) | 5 (25.0) | |
| 60+ | 36 | 32 (52.5) | 4 (20.0) | |
| Years since surgery | ||||
| <1 year | 34 | 15 (24.6) | 19 (95.0) | <0.0001 |
| 1–5 years | 25 | 25 (41.0) | 0 | |
| >5 years | 22 | 21 (34.4) | 1 (5.0) | |
| Years on treatment | ||||
| <1 year | 39 | 19 (31.1) | 20 (100) | <0.0001 |
| 1–5 years | 30 | 30 (49.2) | 0 | |
| >5 years | 12 | 12 (19.7) | 0 | |
All patients receiving taxanes were newly diagnosed
The main output of this instrumental evaluation was the assessment of skin barrier integrity in patients, accounting for several variables: age, time since surgery, and ongoing treatment.
Patients showed well-preserved skin hydration (43.8±8.4 AU) exceeding normative values (39.0±6.9, P<0.001, one-sample t-test) (Table 2).
Age strongly influenced objective parameters: elasticity declined progressively (R2 66.5% [0-49y] to 56.2% [60+], p<0.0001; R5 76.9% to 67.9%, p=0.001), collagen intensity decreased (115.3 to 106.9 AU, p=0.004), roughness increased (Ra 4.9 to 8.0 μm, p<0.0001) (Table 2; Figure 1; Figure 2; Supplementary Figure S1).
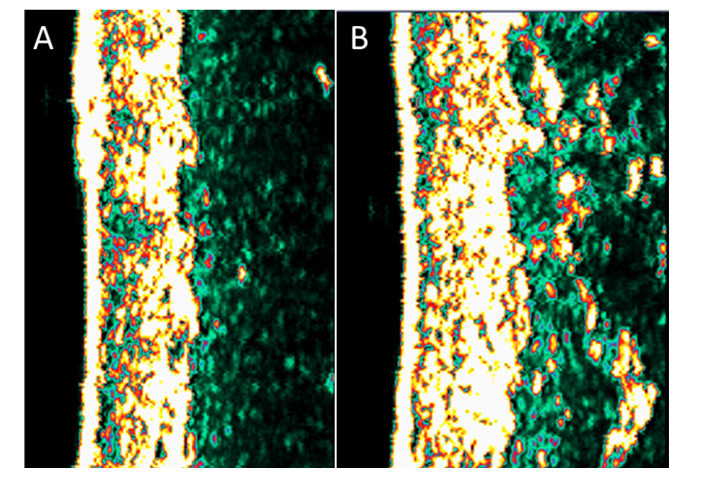
Figure 1:Skin thickness and collagen intensity ultrasound images A) age group 0-49; B) age group 50-59.
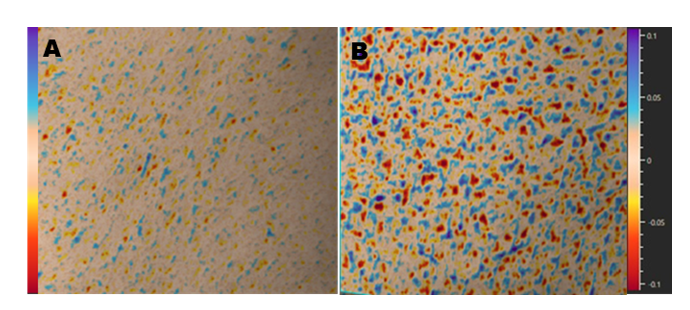
Figure 2:Skin texture and roughness 3D images A) age group 0-49; B) age group 50-59
In the assessment of skin barrier integrity, as measured by transepidermal water loss (TEWL), in the average evaluation on both upper limbs, borderline statistically significant differences were observed between patients receiving aromatase inhibitors (mean TEWL: 12.02±4.5 g/m²h) and those treated with taxanes (mean TEWL: 8.20±2.45 g/m²h; p=0.05). The TEWL values differed significantly according to time from surgery. Patients who had been undergoing treatment for less than 1 year exhibited lower TEWL values (9.32±2.55 g/m²h) in contrast with patients receiving treatment for 1 to 5 years showed the highest TEWL values (13.8±5.95 g/m²h; p=0.02) ( Table 2).
Same results can be observed when hydration and TEWL were measured on the same side as breast cancer or average of both arms in case of bilateral breast cancers (mean TEWL AIs 12.26±4.5 vs taxane 8.19±2.8 g/m²h; p=0.05) and same data during the 1-5 year post-surgical window (mean TEWL 14.14±5.8 g/m²h; p=0.02) compared to patients treated for less than 1 year (9.31±2.7 g/m²h) (Figure 3; Supplementary Table 1s).
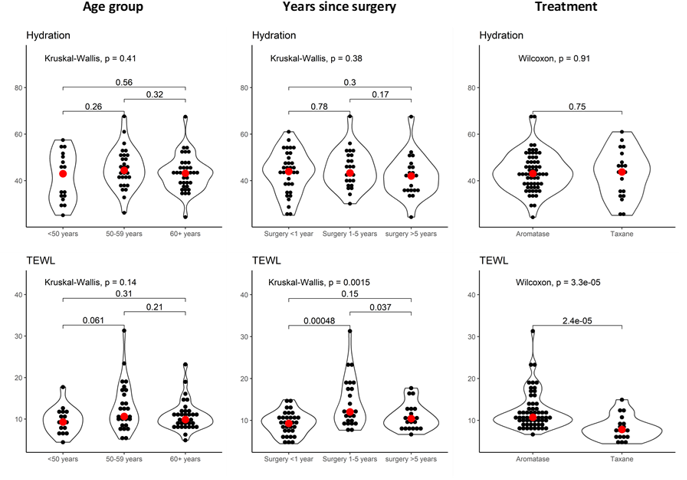
Figure 3:Hydration and TEWL measures on the same side as breast cancer (or average of both arms in case of bilateral breast cancer)
Time since surgery also drove reduced redness variation late (2.46 to 2.56 AU, p=0.03). Multivariable GLM (adjusted for age group, time since surgery, treatment) confirmed age-independence of these trends (TEWL adj-P=0.02; redness variation adj-P=0.03) (Table 2; Figure 4).
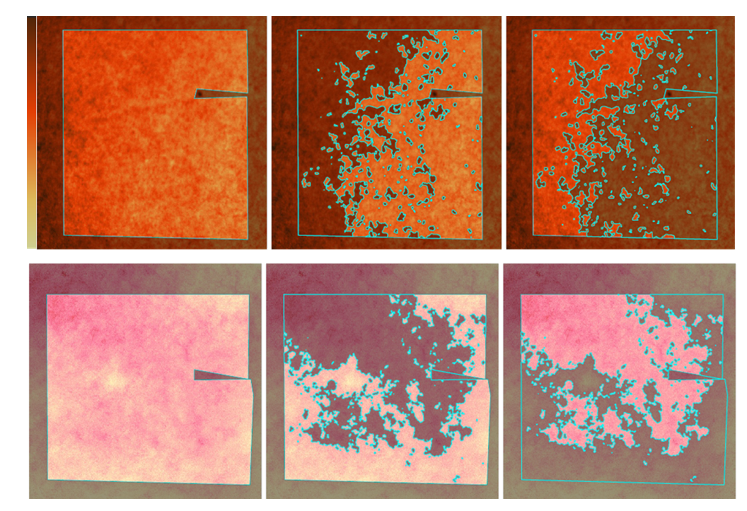
Figure 4:Upper: elaboration of skin pigmentation, Lower: elaboration of skin redness
Treatment differences were modest: taxanes associated with increased dermal thickness (1032 vs 934.8 μm, adj-P=0.002), pigmentation minimum (33.2 vs 29.7 AU, adj-P=0.01), reduced redness minimum (8.1 vs 9.0 AU, adj-P=0.02), and lower redness variation (2.28 vs 2.59 AU, adj-P=0.0004). SkinIndex-29 revealed mild global impairment (28.8±9.7), with comparable symptoms (36.7±15.2), emotions (28.3±11.4), and function (24.2±7.3) across groups (all adj-P>0.05).
Among AIs-treated patients, 20% reported moderate-severe physical symptoms (PS) with 9% experiencing related emotional distress (EM). Taxane recipients showed comparable burden: 23% PS, 11% EM. Functional/social impairment affected 4.5% across groups (all adj-P>0.05).
Discussion
Taxanes compromise skin barrier function through multiple pathways: microtubule stabilization disrupts keratinocyte proliferation/differentiation, downregulates aquaporin-3 (AQP3) and extracellular matrix proteins (COL1, ELN, FN1), and triggers oxidative stress/pro-inflammatory cytokines (IL-6, TNF-α) [23-26]. Aromatase inhibitors (AIs) exert indirect effects via estrogen depletion, impairing estrogen receptor-α/β-mediated regulation of hyaluronic acid synthesis, sebum production, collagen I/III turnover, and keratinocyte growth factor expression critical for epidermal renewal [27-30].
Despite these distinct mechanisms, TEWL showed borderline inter-group differences (AI 12.02±4.5 vs taxane 8.20±2.5 g/m²h; p=0.05), remaining within healthy norms (5-10 g/m²h) except during the 1-5 year post-surgical window (13.81±5.6 g/m²h; p=0.02 vs <1y).
Interestingly, in patients undergoing treatment for more than 5 years, TEWL values appeared to stabilize (10.55 g/m²/h), approaching those observed in the recently treated group.
This triphasic pattern preserved early (<1y: 9.32±2.1), peak intermediate (1-5y), stabilization late (>5y: 10.55±2.8)—diverges from expected cumulative toxicity, suggesting dynamic interplay between treatment burden, behavioral factors, and cutaneous adaptation.
The early preservation likely reflects heightened skincare vigilance post-diagnosis, with regular emollient/barrier-repair use counteracting initial toxicity. Medium-term deterioration aligns with documented compliance decline in chronic disease management, compounded by cumulative endocrine/chemotherapy effects on stratum corneum lipids (ceramide reduction) and corneodesmosome degradation. Late stabilization may indicate cutaneous remodeling residual fibroblasts maintaining baseline collagen turnover or enhanced dermatologic support in long-term survivors.
These findings underline the significance of implementing educational dermatological programs to promote sustained adherence to moisturizing and barrier-protective skincare throughout all steps of cancer treatment.
Early and continuous use of functional dermocosmetics may function as a practical yet straightforward strategy to preserve skin barrier integrity, enhance patient quality of life, and potentially reduce the incidence of dermatologic complications.
Skin texture and roughness were also analyzed in this study. Regarding skin roughness, no statistically significant differences were observed between patients treated with aromatase inhibitors and those receiving taxanes. However, significant variations emerged according to patients’ chronological age, suggesting that aging, rather than treatment type, plays a predominant role in determining skin surface characteristics. Instrumental measurements of Ra values a standard indicator of skin texture revealed a distinct age-dependent profile. Patients aged 0–49 years exhibited a mean Ra of 4.85, significantly lower than the 6.48 observed in the 50–59-year group and the 7.99 in the ≥60-year cohort. By direct comparison, younger patients (0–49) had markedly smoother skin (lower Ra) than both older groups. Moreover, the Rt values, reflecting vertical surface irregularity, followed a comparable age-related trend, increasing from the youngest to the oldest group.
This pattern aligns with published evidence demonstrating that skin surface roughness progressively increases with chronological age, mainly due to intrinsic aging processes such as collagen depletion, elastin disorganization, slowing of epidermal turnover, and a decline in water-retention capacity [31, 32] .
Instrumental data indicate that patients receiving aromatase inhibitors exhibit greater skin redness than those receiving taxane-based therapy. The distinct underlying pathophysiological mechanisms can explain this difference. In patients treated with aromatase inhibitors, redness primarily reflects a vasomotor manifestation secondary to estrogen deprivation. The pathophysiology of hot flushes is unclear; however, estrogen withdrawal clearly plays an important role. It is postulated that declining estrogen levels may alter brain neurotransmitter activity and destabilize the hypothalamic thermoregulatory center [33].
Emerging evidence suggests that estrogen-sensitive hypothalamic neurons expressing estrogen-sensitive neuropeptides may contribute to the thermoregulatory dysfunction of vasomotor symptoms (VMS) by controlling the release of GnRH. Deficient estrogen levels result in unopposed and increased activation of neurons that signal to the hypothalamic thermoregulatory control center. This results in activation of heat-dissipation mechanisms, vasodilation, and sweating, which are experienced as VMS [34].
Conversely, in patients undergoing taxane therapy, skin redness appears to be associated with inflammatory processes and vasodilation mediated by the release of pro-inflammatory mediators. Paclitaxel causes many adverse effects on the skin through several mechanisms. It is directly cytotoxic to keratinocytes, causing type I and IV hypersensitivity reactions that affect, among other tissues, the skin. Another mechanism of toxicity is the inhibition of Bcl-2 expression, an increase in p53 and p21 expression, a decrease in vascular endothelial growth factor (VEGF), an increase in markers of oxidative stress and proinflammatory markers, a decrease in markers of elasticity, and increased pigment production in melanocytes [35]. According to mechanisms described in the literature, it may be hypothesized that in patients treated with aromatase inhibitors, cutaneous flushing is frequent because the significant reduction in estrogen levels alters hypothalamic thermoregulation and peripheral vasodilation, leading to hot flashes like those observed during menopause. In contrast to taxanes, flushing is not a typical manifestation; when present, it is usually acute and related to infusion-associated hypersensitivity reactions rather than a chronic hormonal mechanism.
In addition to redness, instrumental analyses were also performed on skin pigmentation and thickness. Instrumental analyses revealed taxane-specific increases in dermal thickness (1032±148 vs 935±128 μm AI, adj-P=0.002) and pigmentation minimum (33.2±5.1 vs 29.7±4.2 AU, adj-P=0.01), consistent with taxane-induced sclerodermoid fibrosis (TGF-β/myofibroblast activation) and melanogenesis (paclitaxel activates MITF/ERK and increases melanin content)[12]. These structural changes contrast AI estrogen-depletion effects, yet both contribute to subtle, non-CTCAE detectable dAEs.
This discrepancy between patient-reported outcomes and objective findings highlights an important methodological and clinical consideration: each tool provides a distinct perspective on the dermatological experience. The Skindex-29 captures the patient’s subjective perception, which may be influenced by personal, contextual, or treatment-related factors, whereas instrumental techniques yield standardized, reproducible, and clinically quantifiable data.
Supporting this interpretation, patients undergoing chemotherapy, commonly perceived as a more invasive treatment, reported greater concern regarding the persistence or worsening of symptoms compared to those receiving endocrine therapy. This discrepancy does not constitute a contradiction but instead underscores the importance of integrating both perspectives.
From a clinical perspective, relying solely on instrumental data may result in an underestimation of patients' subjective discomfort, especially in populations undergoing prolonged or emotionally challenging treatments. On the other hand, using only questionnaires might lead to an overestimation of the clinical significance of minor or temporary skin changes. By employing a combined assessment strategy, healthcare providers can align subjective perceptions with the underlying pathophysiology, ultimately improving clinical management and enhancing communication with patients.
Previous studies have reported similar findings, highlighting the importance of integrating objective skin measurements with patient-reported outcomes when evaluating dermatologic toxicity in oncology care. [36, 37].
Conclusion
The study measured objective outcomes, affected by the time frame and/or therapy, and subjective data related to patient quality of life, providing preliminary objective skin parameters in oncological patients undergoing different pharmacological therapies.
Based on the results, it is not possible yet to definitively establish a difference between the groups that underwent different treatments.
Age and time since surgery predominate over adjuvant therapy type and a distinctive triphasic TEWL pattern—early preservation (<1y), peak deterioration (1-5y), late stabilization (>5y)—suggesting cutaneous adaptation modulated by skincare adherence rather than cumulative toxicity.
Taxanes were associated with increased dermal thickness (1032 vs 935 μm, adj-P=0.002) and pigmentation alongside reduced redness heterogeneity versus aromatase inhibitors, while Skindex-29 revealed comparable mild global impairment (28.8±9.7) across groups, highlighting discrepancies between objective measures and patient-reported burden that necessitate integrated assessments in supportive oncology.
These findings advocate implementation of longitudinal dermatologic education programs emphasizing continuous emollient/barrier-repair use particularly during the vulnerable 1-5 year post-surgical window to optimize skin homeostasis, enhance quality of life, and mitigate underrecognized dermatologic adverse events throughout breast cancer survivorship.
Authors’ Contributions
Conception and design
Emanuela Omodeo Salé, Monica Iorfida, Paola Perugini, Collection and assembly of data: Paola Perugini, Camilla Ottomano, Maria Vittoria Visconti, Matilde Monteleone; Data analysis and interpretation: Patrick Maisonneuve; Manuscript writing/final approval of the manuscript: All authors.
Funding
This work was partially supported by the Italian Ministry of Health with Ricerca Corrente and 5 × 1000 funds.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This trial was approved by IEO Institutional Review Board (project code: UID 4588/12_March_2024). All patients provided written informed consent before the initiation of the study.
Consent for Publication
All authors have provided their consent for publication
Competing Interests
The authors declare no conflicts of interest
Acknowledgements
Not applicable.
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. doi:10.3322/caac.21834.
2. Giaquinto AN, Sung H, Newman LA, Freedman RA, Smith RA, Star J, Jemal A, Siegel RL. Breast cancer statistics 2024. CA Cancer J Clin. 2024;74(6):477-495. doi:10.3322/caac.21863.
3. Bhatia N, Thareja S. Aromatase inhibitors for the treatment of breast cancer: An overview (2019–2023). Bioorg Chem. 2024;151:107607. doi:10.1016/j.bioorg.2024.107607.
4. Janni W, Hepp P. Adjuvant aromatase inhibitor therapy: outcomes and safety. Cancer Treat Rev. 2010;36(3):249-261. doi:10.1016/j.ctrv.2009.12.010.
5. Wu YY, Huang QL, Luo ZY, et al. Evaluation of dermatologic adverse events associated with aromatase inhibitors: insights from the FAERS database. Front Pharmacol. 2025;16:1529342. doi:10.3389/fphar.2025.1529342.
6. Czajka-Oraniec I, Simpson ER. Aromatase research and its clinical significance. Endokrynol Pol. 2010;61(1):126-134.
7. Lephart ED, Naftolin F. Menopause and the skin: old favorites and new innovations in cosmeceuticals for estrogen-deficient skin. Dermatol Ther (Heidelb). 2021;11(1):53-69. doi:10.1007/s13555-020-00468-7.
8. Lai JI, Chao TC, Liu CY, Huang CC, Tseng LM. A systematic review of taxanes and their side effects in metastatic breast cancer. Front Oncol. 2022;12:940239. doi:10.3389/fonc.2022.940239.
9. Henderson IC, Berry DA, Demetri GD, Cirrincione CT, Goldstein LJ, Martino S, et al. Improved outcomes from adding sequential paclitaxel but not from escalating doxorubicin dose in an adjuvant chemotherapy regimen for patients with node-positive primary breast cancer. J Clin Oncol. 2003;21(6):976-983. doi:10.1200/JCO.2003.02.063.
10. Swain SM, Jeong JH, Geyer CE Jr, Costantino JP, Pajon ER, Fehrenbacher L, et al. Longer therapy, iatrogenic amenorrhea, and survival in early breast cancer. N Engl J Med. 2010;362(22):2053-2065. doi:10.1056/NEJMoa0909638.
11. Donati A, Castro LG. Cutaneous adverse reactions to chemotherapy with taxanes: the dermatologist's point of view. An Bras Dermatol. 2011;86(4):755-758.
12. Sibaud V, Lebœuf NR, Roche H, et al. Dermatological adverse events with taxane chemotherapy. Eur J Dermatol. 2016;26(5):427-443. doi:10.1684/ejd.2016.2833.
13. Dasanu CA, Alexandrescu DT. Systemic lupus erythematosus associated with paclitaxel use in the treatment of ovarian cancer. South Med J. 2008;101(11):1161-1162. doi:10.1097/SMJ.0b013e31818956f6.
14. Verdelli A, Antiga E, Bonciani D, et al. Docetaxel-induced subacute cutaneous lupus erythematosus. Clin Exp Dermatol. 2016;41(3):318-319. doi:10.1111/ced.12756.
15. Perry N, Broeders M, de Wolf C, Tornberg S, Holland R, von Karsa L, editors. European guidelines for quality assurance in breast cancer screening and diagnosis. 4th ed. Luxembourg: Office for Official Publications of the European Communities; 2006.
16. National Breast Cancer Coalition (NBCC). 2nd annual breast cancer deadline 2020 progress report. Washington (DC): NBCC; Available from: http://www.breastcancerdeadline2020.org/
17. Chren MM. The Skindex instruments to measure the effects of skin disease on quality of life. Dermatol Clin. 2012;30(2):231-236. doi:10.1016/j.det.2011.11.003.
18. Abeni D, Damiano A, et al. Further evidence of the validity and reliability of the Skindex-29: an Italian study on 2242 dermatological outpatients. Dermatology. 2002;204(1):43-49. doi:10.1159/000051809.
19. Barbu MA, Nițipir C, Voiosu T, Giurcăneanu C. Impact of dermatologic adverse reactions on quality of life in oncologic patients. Rom J Intern Med. 2018;56(2):96-101. doi:10.2478/rjim-2018-0002.
20. Blichmann CW, Serup J. Assessment of skin moisture: measurement of electrical conductance, capacitance and transepidermal water loss. Acta Derm Venereol Suppl (Stockh). 1988;68:284.
21. Seck A, Dee H, Smith W, Tiddeman B. 3D surface texture analysis of high-resolution normal fields for facial skin condition assessment. Skin Res Technol. 2020;26(2):169-186. doi:10.1111/srt.12793.
22. Neto P, Ferreira M, Bahia F, Costa P. Improvement of methods for skin mechanical properties evaluation through correlation between different techniques and factor analysis. Skin Res Technol. 2013;19:405-416.
23. Montero P, Pérez-Leal M, Pérez-Fidalgo JA, et al. Paclitaxel induces epidermal molecular changes and produces subclinical alterations in the skin of gynecological cancer patients. Cancers (Basel). 2022;14(5):1146. doi:10.3390/cancers14051146.
24. Jordan MA, Wilson L. Microtubules as a target for anticancer drugs. Nat Rev Cancer. 2004;4(4):253-265. doi:10.1038/nrc1317.
25. Montero P, Milara J, Pérez-Leal M, et al. Paclitaxel-induced epidermal alterations: an in vitro preclinical assessment in primary keratinocytes and in a 3D epidermis model. Int J Mol Sci. 2022;23(3):1142.
26. Pelletier G, Ren L. Localization of sex steroid receptors in human skin. Histol Histopathol. 2004;19(2):629-636. doi:10.14670/HH-19.629.
27. Kumar MM, Davuluri S, Poojar S, Mukherjee G, Bajpai AK, Bafna UD. Role of estrogen receptor alpha in human cervical cancer-associated fibroblasts: a transcriptomic study. Tumour Biol. 2016;37(4):4409-4420. doi:10.1007/s13277-015-4257-6.
28. Creidi P, Faivre B, Agache P, Richard E, Haudiquet V, Sauvanet JP. Effect of a conjugated oestrogen cream on ageing facial skin: a comparative study with a placebo cream. Maturitas. 1994;19(3):211-223. doi:10.1016/0378-5122(94)90074-4.
29. Irrera N, Pizzino G, D’Anna R, Vaccaro M, Arcoraci V, Squadrito F. Dietary management of skin health: the role of genistein. Nutrients. 2017;9(6):622. doi:10.3390/nu9060622.
30. Wilkinson HN, Hardman MJ. The role of estrogen in cutaneous ageing and repair. Maturitas. 2017;103:60-64. doi:10.1016/j.maturitas.2017.06.026.
31. Meng H, Lin W, Dong Y, et al. Statistical analysis of age-related skin parameters. Technol Health Care. 2021;29(S1):65-76. doi:10.3233/THC-218007.
32. Bachmann GA. Menopausal vasomotor symptoms: a review of causes, effects and evidence-based treatment options. J Reprod Med. 2005;50(3):155-165.
33. Sibaud V, Lebœuf NR, Roche H, et al. Dermatological adverse events with taxane chemotherapy. Eur J Dermatol. 2016;26(5):427-443. doi: 10.1684/ejd.2016.2833.
34. Atwell K, White M, Kuphal G, Williams M, Schrager S. Treatment of vasomotor symptoms. J Am Board Fam Med. 2024;37(5):923-932. doi:10.3122/jabfm.2023.230408R1.
35. Nižnanský Ľ, Osinová D, Kuruc R, Hengerics Szabó A, Szórádová A, Masár M, Nižnanská Ž. Natural taxanes: from plant composition to human pharmacology and toxicity. Int J Mol Sci. 2022;23(24):15619. doi:10.3390/ijms232415619.
36. Bottesi G, Stefanelli A, Ambroso G, et al. The relevance of assessing subjective experiences of skin toxicity during adjuvant radiotherapy for breast cancer. Front Oncol. 2021;11:645921. doi:10.3389/fonc.2021.645921.
37. Almeida V, Pires D, Silva M, et al. Dermatological side effects of cancer treatment: psychosocial implications—a systematic review of the literature. Healthcare (Basel). 2023;11(19):2621. doi:10.3390/healthcare11192621.
Received: March 23, 2026;
Accepted: April 16, 2026;
Published: April 22, 2026
.
To cite this article : Iorfida M, Visconti MV, Monteleone M, Ottomano C, Tosti G, Rojas DP, et al. Biophysical skin parameters and skin related quality of life in breast cancer patients. Br J Cancer Res. 2026;9(1):859–868. doi:10.31488/bjcr.216.
© The Author(s) 2026. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).