Review article / Open Access
DOI: 10.31488/bjcr.172
PhiΦ Breast New Diagnostic Techniques for Breast Cancer Detection
Ersilio Trapanese MD*1,2, Giulio Tarro, MD, PhD3
1. Director from Division of Diagnostic Imaging & Interventional Ultrasound - CMM Diagnostic Center - Cava de’ Tirreni, Italy
2. Member of the Board of Directors T. & L. De Beaumont Bonelli Foundation for Cancer Research - Nap les, Italy
3. President Foundation T. & L. De Beaumont Bonelli for Cancer Research - Naples, Italy
*Corresponding author: Trapanese E, Member of the Board of Directors T. & L. De Beaumont Bonelli Foundation for Cancer Research - Naples, Italy, Tel: +390815463222.
Abstract
Today, breast cancer is one of the most aggressive cancers in women and new cases continue to increase worldwide. In order to reduce mortality we need to detect this life threatening disease at an earlier stage. We have conducted a study for the identification and characterization of suspicious breast lesions using a new diagnostic technique applied to ultrasonography and mammography called “PhiΦBreast.” Identification and characterization of category C4-C5 lesions of the breast with high Predictive Positive PPV value, with a new innovative method called “PhiΦBreast” using the Golden Ratio (Phi, or Φ 1.618...) Fibonacci sequence and a Predictive Algorithm, applied to the ultrasonography and mammography with subsequent deepening with cytological examination using Fine Needle Aspiration Cytology (FNAC), according to evaluation criteria of the Breast Imaging Report Data System (BI-RADS) and the American College of Radiology (ACR). Usefulness of this research and the use of this new diagnostic tecnique is to detect the breast cancer in early stage. In addition to develop a classification model of the histological type identified in the section areas and the percentage of probability in relation between the Golden Ratio (Φ) and Fibonacci sequence. This amazing intuition and research has given contribution to the new Theory of Spiral Cancer. This innovative diagnostic technique has shown a sensitivity of 95%, a specificity of 97%, a positive predictive value (PPV) of 97%, and negative predictive value (NPV) of 96%. Furthermore with a Predictive Algorithm associated with malignant cytology after FNAC, we have classified different types of potentially life threatening cancers for patients.
Keywords: PhiΦBreast, predictive algorithm, golden ratio, fibonacci sequence, breast cancer
Introdution
Breast cancer is the most commonly diagnosed cancer among US women. With an estimated 268,600 newly diagnosed women with invasive disease, 48,100 cases of ductal carcinoma in situ (DCIS) in 2019, accounting for approximately 15.2%-30% of all new cancer cases among women, with the mortality rate of 16%.
The highest incidence is recorded in North America with 90 cases per 100,000 women [1,2]. In Europe, every year more than 200,000 women are affected by breast cancer every year, with an incidence ranging from 5 to 10% depending on the country.
There are several risk factors that contribute to the development of breast cancer. Most relevant non-changeable risk factors are: gender, age, genetic predisposition, mutations in the BRCA1, BRCA2 genes [3] (which carry a 60-90% risk of developing a breast cancer over the course of life), Li Fraumeni syndrome [4], mutation of the gene that codes for p53 [5], Lynch syndrome [6]. Ethnic group [7], atypical mammary hyperplasia, high breast density. Environmental factors: exposure to ionizing radiation in childhood and / or juvenile age (for example in women with previous Hodgkin lymphoma). Hormonal therapies: HRT-estroprogestinic [8], which involve a minimum increased risk. In our research, nodular lesions of the breast category C4-C5 with high positive predictive value (PPV), were identified and characterized with a new method called PhiΦBreast using the Golden Ratio, Fibonacci sequence and a Predictive Algorithm, applied to ultrasonography and mammography with subsequent study with cytological examination using fine needle aspiration cytology (FNAC) in respecting the criteria of the American College of Radiology (ACR) and Breast Imaging Report Data System (BI-RADS).
Methods
For two years, we have conducted a study for the identification and characterization of suspicious breast lesions using a new diagnostic technique applied to ultrasonography and mammography called “PhiΦBreast.” All patients underwent to two-dimensional ultrasound examination (2 DUS). The acquired dynamic image sequences were digitally stored on the ultrasound system Mindray M9 (Nanshan, Shenzhen, P.R. China) using a high-frequency 13 MHz linear probe.
High-resolution real-time ultrasonography (US) can detect characteristics of breast nodules. Characterization of the mammary nodules was performed according to the following criteria: shape, echostructure, level of echogenicity, margins, size and topographical area. Using the method of PhiΦBreast ultrasonographic study, on 55/987 patients were identified solid lesions markedly hypoechoic echostructure, round shape, with irregular and infiltrative margins and cuneiform shape with blurred margins (Figure 1).
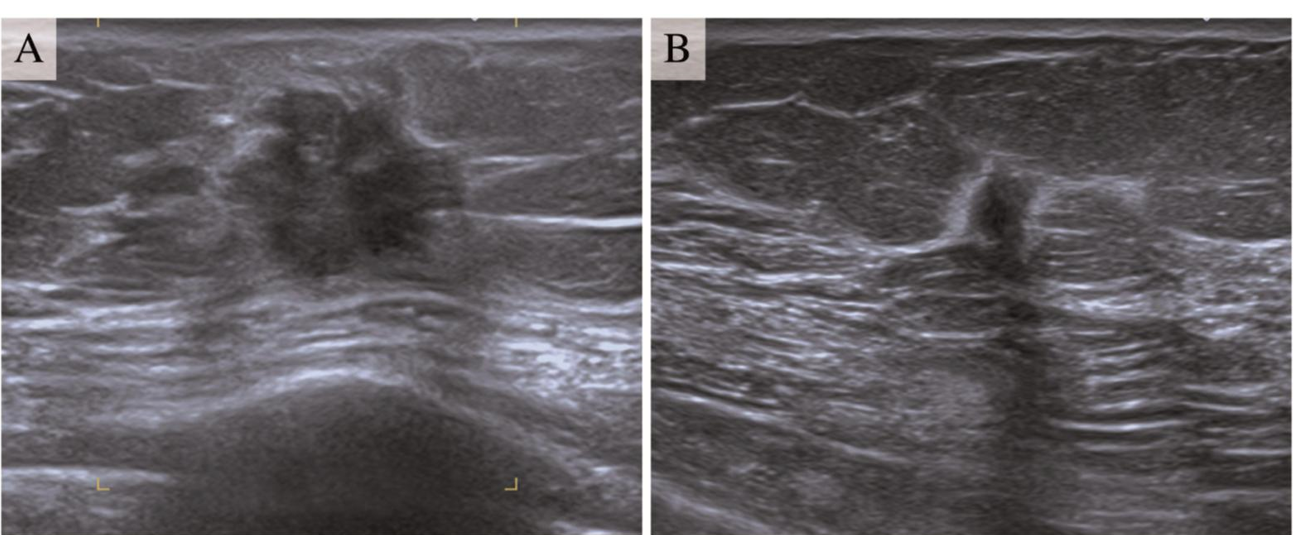
Figure 1:Ultrasonography Image Of Suspicious Nodular Lesions Identified With PhiΦBreast Model Panel A solid lesion, round shape, markedly hypoechoic echostructure with irregular and infiltrative margins. Panel B solid lesion, cuneiform shape, markedly hypoechoic echostructure with
After having their consent, 55 selected patients underwent a mammography examination with subsequent diagnostic deepening Fine Needle Aspiration Cytology (FNAC) procedure under ultrasonography guidance. PhiΦBreast imaging applied to the mammography in the craniocaudal (CC) view and mediolateral oblique (MLO) view has given rise to a mapping of neoplastic nonpalpable breast lesions (Figure 2 and Figure 3). PhiΦBreast produced important data for the elaboration of a Predictive Algorithm on the probability of development of various histological types of tumors and the percentage detectable in the areas of the Golden Ratio and the Fibonacci numbers, when applied in the breast (13,21,34,55,89,144) using the following nomenclature "Fibonacci-number Side" (FS1,FS2,FS3,FS4,FS5,FS6) (Table 1).
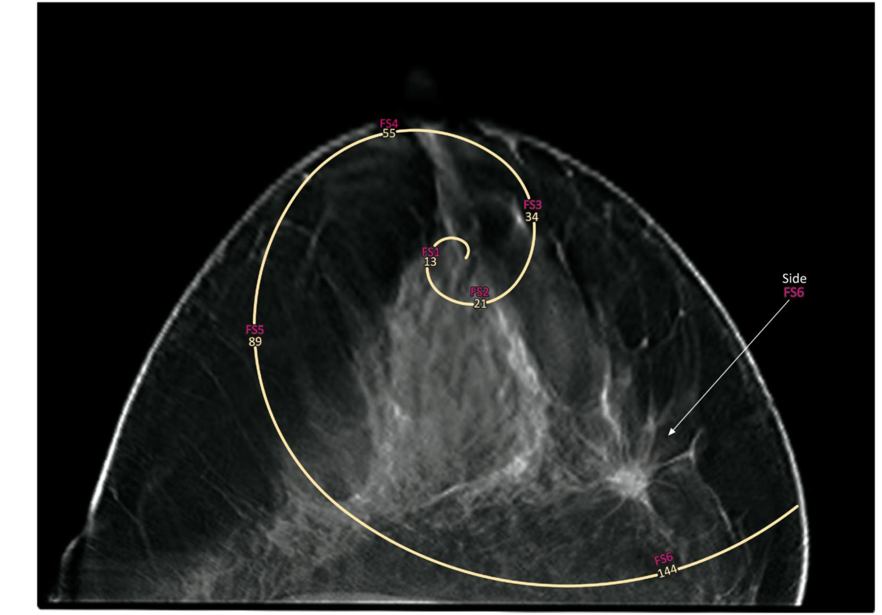
Figure 2:Golden Ratio (Φ) Breast Cancer Detection And Fibonacci Sequence Cranial-caudal view (CC) show Fibonacci Spiral approximates the Golden Ratio (Φ) using mammogram inscribed in squares of integer Fibonacci number side, shown for square size (13,21,34,55,89,144) making use the following nomenclature "Fibonacci- number Side” (FS1,FS2,FS3,FS4,FS5,FS6). The arrow show extraordinary X-ray vision of the cancer accurately detected in FS6 side.
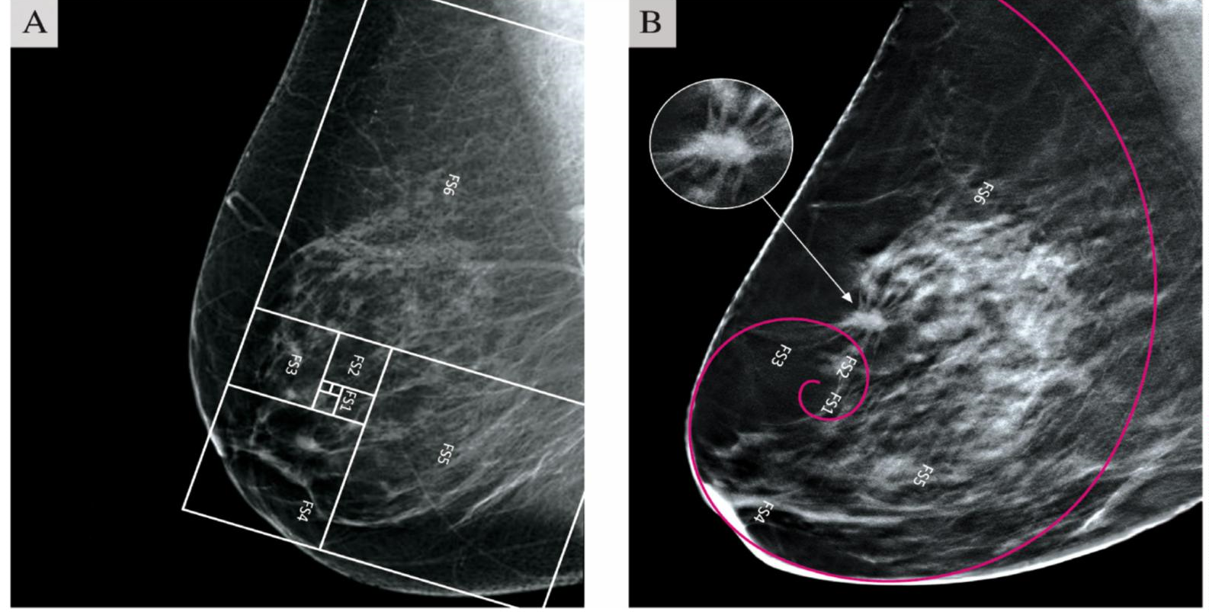
Figure 3:PhiΦBreast A New Diagnostic Technique for Breast Cancer Detection Panel A show mediolateral oblique view (MLO) of the breast at mammographic X-ray with applied Golden Ratio and Fibonacci numbers of healthy individual. No nodules were detected along the Golden Ratio. Panel B PhiΦBreast imaging applied to the mammogram has provided a mapping of neoplastic lesion. White arrow highlights cancerous tumor detected in FS6 side of the Golden Spiral. Cancerous mass appear as a bright and irregular image with spiky edges
The results of cytology identified 55 tumors:13 ductal carcinomas in situ, 10 invasive ductal carcinomas, 6 invasive lobular tumors and 26 invasive carcinomas not otherwise specified. The surgery was established based on the type of tumor identified in patients in the preoperative phase. The histological diagnosis confirmed the tumor nature of the cells of the analyzed tissues, performed according to the criteria established by the American College of Radiology (ACR) and Reporting Breast Imaging and Data System (BI- RADS). Patients underwent blood chemistry controls and tumor markers. The follow up period lasted about 1 year.
Table 1:Predictive Algorithm Breast Cancer
| Histological Types and percentages tumors detected in the Golden Ration (φ) and Fibonacci sequence | |
|---|---|
| φSection Area 13 | *FS1 Ductal Carcinomas in Situ [ 3%] |
| φSection Area 21 | *FS2 Ductal Carcinomas in Situ [7%] |
| φSection Area 34 | *FS3 Invasive Ductal Carcinomas [13%] |
| φSection Area 55 | *FS4 Invasive Ductal Carcinomas [8%] |
| φSection Area 89 | *FS5 Invasive Lobular Tumors [14%] |
| φSection Area 144 | *FS6 Invasive Ductal Carcinomas not Otherwise Specified [55%] |
φGolden Ratio and the Nomenclature *Fibronacci-number Side
Percentage of tumors detected in the Fibronacci-number Side: FS1-FS2 10% of ductal carcinomas in situ; FS3-FS4 21% of
invasive ductal carcinomas; FS5 14% invasive lobular tumors and FS6 55% invasive carcinomas not otherwise specified.
Results
The Golden Ratio (Phi, or Φ 1.618...) is a potentially unifying quantity of structure and function in nature, as best observed in phyllotactic patterns in plants. For centuries, Phi (Φ) has been identified in human anatomy, and in recent decades, Φ has been proved in human physiology as well with scientific studies of some authors [9,10]. With the use of Golden Ratio [11] and Fibonacci sequence [12] applied to ultrasonography and mammography, we have experimented and developed a diagnostic map with characteristics of high probability of identifying suspicious lesions at an early stage.
We examined 987 women, 55 lesions detected with PhiΦBreast pattern were classified according to BI-RADS descriptors for US-imaging, including morphologic features that had a high predictive value for the malignancy (p<0.001).
This innovative diagnostic technique has shown a sensitivity of 95%, a specificity of 97%, a positive predictive value (PPV) of 97%, and negative predictive value (NPV) of 96%. The discriminating capacity of PhiΦBreast was significantly better than normal ultrasonography (P < 0,05). Furthermore with a Predictive Algorithm associated with malignant cytology after FNAC, we have classified different types of potentially life threatening cancers for patients. It has been hypothesized to develop a theory of spiral cancer cell growth, called The Theory of Spiral Cancer [13].
Discussion
Fascinated by golden ratio and Fibonacci sequence, we have devised a new diagnostic imaging model called PhiΦBreast applied to ultrasonography and mammography to early detection nodular lesions with echostructural features of malignancy. The National Cancer Institute (NCI) recommends five categories for diagnosis of breast aspiration cytology [14] in order to bring a degree of uniformity to the diagnostic repoting. These categories are unsatisfactory (C1), benign lesion (C2), atypical, probably benign (C3), suspicious, probably malignant (C4), and malignat (C5). However, some authors believe that C3 and C4 should be categorized in the same category [15,16].
The analyzed cytological samples were classified according to NHSBSP into the following categories: C4-C5 [17]. A modern predictive algorithm and a theoretical model of spiral cancer growth has been elaborated. We have used a Mindray M9 ultrasound system with high frequency probes was used, 10-15 MHz for the study of echostructural changes in the breast.
After considerable study on 987 patients, 55 nodular lesions were identified using the PhiΦBreast ultrasonography method for topographic mapping and taking into consideration the following ultrasound features: shape, echostructure, level of echogenicity, margins, size and topographical area. Lesions detected showed two forms with an markedly hypoechoic echostructure: round shape with irregular and infiltrative margins and cuneiform shape with blurred margins.All features with high predictive value for malignancy (p < 0.001).
This diagnostic technique called PhiΦBreast in ultrasonography and mammography, respecting the criteria of the American College of Radiology (ACR) [18] & Breast Imaging Report Data System (BI-RADS) [19] proved to be reliable. Having compared our research with important magnetic resonance imaging (MRI) studies performed by various researchers [26,27,28,29,30], the early identification of malignant lesions was confirmed, with a high positive predictive value (PPV) with a sensitivity (95%) specificity (97%) value positive predictive (97%) negative predictive value (96%).
We selected 55 patients, which were subjected to a diagnostic deepening with mammography exam and used as a reading interpretation to mammogram the PhiΦBreast imaging method and subsequent FNAC [20] under ultrasound guidance with a 19 gauge needle by execution of three passages through the nodular lesion.
Suspicious lesions detected from topographic mapping were classified category C4-C5 (NCI guidelines) [21]. The surgical procedure was decided after preoperative phase based on the result of the BI-RADS cytological classification and contrast medium MRI of the breast and axillary limph nodes (LMN).
Patients were treated with different surgical techniques. The Veronesi quadrantectomy [22] represents a milestone in the treatment of breast cancer, currently the first scientifically validated conservative protocol. The Nipple Sparing Mastectomy (NSM) [23], the Skin-Sparing Mastectomy that includes the Nipple-Areolar Complex (SSM+NAC) [24] with lymphadenectomy and Intraoperative Radiation Teraphy (IORT) [25]. Post-operative histological results were all classified as carcinomas.
We paid special attention to the ability of PhiΦBreast to offer an innovative topographic diagnostic imaging of suspicious lesions and using a predictive algorithm. Different types of tumors were detected in the Golden Section areas, using Fibonacci numbers for mapping and classify the percentage of cancers identified in the different sections.
Percentage of tumors detected in the Fibonacci-number side was as follows: FS1-FS2 (10%) of ductal carcinomas in situ; FS3-FS4 (21%) of invasive ductal carcinomas; FS5 (14%) invasive lobular tumors and FS6 (55%) invasive carcinomas not otherwise specified. These identified lesions had a high predictive value for malignancy (p <0.001).
A meticolous study was also performed on the echostructural characteristics of the lesions identified by this mapping. It has shown validating that the irregular and spiculated margins are associated with greater probability of malignancy, as also described by other authors. Liberman et al. [26] described in a study that a spicular margin was the most suspicious characteristic identified with a high PPV. Wedegärtner et al. [27] reported an irregular margin of the lesion to be the most reliable morphological feature to indicate malignancy.
Schnall and colleagues [28] identified spiculated margins to be a highly predictive feature of the cancer image and Gutierrez et al. [29] found irregular or spiculated margins conferring the highest probability of malignancy by BI-RADS classification. In a retrospective study, Tozaki and collaborators [30] found irregular shape (97%) and spiculated margins (100%) among the features with higher predictive value for carcinoma. In relation to these important results, we believe that the nodular lesions identified at an early stage and using this innovative PhiΦBreast imaging method were found to be strongly associated with malignancy (p <0.001) and with high PPV: 97%.
Conclusion
Availing Golden Ratio (Φ), Fibonacci sequence and Predictive Algorithm applied to ultrasonography and mammography, we have given rise to a new diagnostic imaging model called PhiΦBreast for the identification of category C4-C5 lesions with high PPV in respecting the criteria of the American College of Radiology (ACR) and Breast Imaging Reporting Data System (BI-RADS).
This original scientific paper could bring progress in science, an important advancement and discovery which could save more lives from despair and in the worst case scenario of the patient's death. Early diagnosis is essential because it allows the removal of small tumors and therefore able to produce more limited metastases compared to the potential growth of larger tumors. PhiΦBreast could have important diagnostic imaging applications as a new strategy for thwart breast cancer.
Acknowledgments
The authors thank for their support: Foundation T. & L. De Beaumont Bonelli for Cancer Research - Naples - Italy.
CMM Diagnostic Center - Italy.
Author’s Contributions
This work was carried out in collaboration among with the authors. Author ET prepared and wrote the manuscript, conceived imaging, developed concept and ideas by PhiΦBreast Model. Author GT contributed the supervision of the manuscript.
Funding
No funding was received.
Availability of Data and Materials
The datasets used during the present study are available from the corresponding author upon reasonable request.
Declarations
Ethics approval and consent to participate
All authors hereby declare that all experiments have been examined and approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Consent for publication not applicable.
Competing Interests
The authors declare that they have no competing interests.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics 2015. CA Cancer J Clin. 2019;69 (1):7-34.
2. Statistical Research and Applications Branch, National Cancer Institute. DevCan: Probability of Developing or Dying of Cancer. DevCan software,version 6.7.3.(2015).Statistical Research and Applications Branch, National Cancer Institute.
3. Narod SA, Salmena L. BRCA1 and BRCA2 mutations and breast cancer. Discov Med 2011;12:445-53.
4. Ariffin H, et al. Whole-genome sequencing analysis of phenotypic heterogeneity and anticipation in Li-Fraumeni cancer predisposition syndrome Proc Natl Acad Sci.2014. USA.111: 15497-15501.
5. Leroy B, et al. The TP53 website:an integrative resource centre for the TP53 mutation database and TP53 mutant analysis .Nucleic Acids Res. 2013; 41:D962 – D969.
6. Barrow E, Hill J, Evans DG. Cancer risk in Lynch Syndrome. Fam. Cancer. 2013;12:229 - 240.
7. Chlebowski RT, Chen Z, Anderson GL, et al. Ethnicity and breast cancer: factors influencing differences in incidence and outcome. J Natl Cancer Inst. 2005;97:439-448.
8. Fletcher AS, Erbas B, Kavanagh AM, et al. 2005;14:192–200.
9. Tamargo RJ, Pindrik JA. Mammalian Skull Dimensions and Golden Ratio. J Craniofac Surg 2019;30: 1750-1755.
10. Yetkin G, Sivri N, Yalta K, et al. Golden Ratio is beating in our heart. Int J Cardiol. 2013; 168:4926–4927.
11. Livio M. The Golden Ratio: The Story of Phi, the World’s Most Astonishing Number. New York, NY: Broadway Books, Random House Inc; 2002.
12. Vajda S. Fibonacci and Lucas numbers, and the Golden section: theory and applications. Dover Publication 2008;New York, NY.
13. Trapanese E, Tarro G. PhiΦBreast & Theory of Spiral Cancer New Diagnostic Techniques For Breast Cancer Detection. Transl Med Commun.2021;6:23.
14. The uniform approach to breast fine-needle aspiration biopsy. National Cancer Institute Fine-Needle Aspiration of Breast Workshop Subcommittees. Diagnostic Cytopathol. 1997; 16: 295-311.
15. Howell LP. Equivocal diagnoses in breast aspiration biopsy cytology: sources of uncertainty and the role of, “atypical/indeterminate terminology.” Diagnostic Cytopathol. 199; 21:217-222.
16. Kanhoush R, Jorda M, Gomez-Fernandez C, et al. Atypical and “suspicious” diagnoses in breast aspiration cytology: is there a need for two categories? Cancer. 2004; 102: 164-167.
17. Kocjan G. Needle aspiration cytology of the breast: current perspective on the role in diagnosis and management. Acta Med Croatica. 2008;62(4)391-401.
18. Mainiero MB, Moy L, Baron P, et al. ACR Appropiateness Criteria Breast Cancer Screening. J Am Coll Radiol. 2017;14(11S):S383-S390.
19. Berg WA, Campassi C, Langenberg P, et al. Breast Imaging Reporting and Data System Inter-and Intraobserver Variability in Feature Analysis and Final Assessment. AJR Am J Roentgenol. 2000;174(6):1769-77.
20. Yu YH, Wei W, Liu JL. Diagnostic value of fine-needle aspiration biopsy for breast mass: A systematic review and meta-analysis. BMC Cancer. 2012;12:41.
21. Arul P, Suresh M. Application of National Cancer Institute recommended terminology in breast cytology. J Cancer Res Ther.2017;13(1):91-96.
22. Zurrida S, et al. The Veronesi quadrantectomy: an established procedure for the conservative treatment of early breast cancer. Int J Surg Investig. 2001;2(6):423–31.
23. Crowe JP Jr, Kim JA, Yetman R, et al. Nipple-sparing mastectomy: technique and results of 54 procedures. Arch Surg. 2004;139:148–150.
24. Gerber B, Krause A, Reimer T, et al, Skin-sparing mastectomy with conservation of the nipple-areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg. 2003;238:120–127.
25. Sedlmayer F, Reitsamer R, Wenz F, et al, Intraoperative radiotherapy (IORT) as boost in breast cancer. Radiat Oncol. 2017;12:23.
26. Liberman L, Morris EA, Lee MJ-Y, et al. Breast lesions detected on MR imaging: features and positive predictive value. AJR Am J Roentgenol. 2002;179(1):171–178.
27. Wedegärtner U, Bick U, Wörtler K, et al. Differentiation between benign and malignant findings on MR-mammography: usefulness of morphological criteria. Eur Radiol. 2001;11(9):1645–1650.
28. Schnall MD, Blume J, Bluemke DA, et al. Diagnostic architectural and dynamic features at breast MR imaging: multicenter study. Radiol. 2006;238(1):42–53.
29. Gutierrez RL, DeMartini WB, Eby PR, et al. BI-RADS lesion characteristics predict likelihood of malignancy in breast MRI for masses but not for nonmasslike enhancement. AJR Am J Roentgenol. 2009;193(4):994–1000.
30. Tozaki M, Igarashi T, Fukuda K. Positive and negative predictive values of BI-RADS-MRI descriptors for focal breast masses. Magn Reson Med. Sci 2006;5(1):7–15.
Received: December 22, 2021;
Accepted: January 17, 2022;
Published: January 20, 2022.
To cite this article : Ersilio Trapanese, Giulio Tarro. PhiΦ Breast New Diagnostic Techniques for Breast Cancer Detection. British Journal of Cancer Research. 2021; 4(3): 534- 539. doi: 10.31488/bjcr.173
©2021 Ersilio Trapanese.