Case report / Open Access
DOI: 10.31488/bjcr.196
Rare Case of Pancreatic Cancer with Metastasis to the Trapezium
Talwinder Nagi MD1, Raksha Sharma MD2, Elisheva Knopf MS3, Warren Brenner MD4
1. Florida Atlantic University, USA
Abstract
In 2023, there were an estimated 64,050 new cases of pancreatic cancer and 50,550 deaths [10]. A diagnosis of metastatic pancreatic cancer has an extremely poor prognosis, with a five-year survival rate of about 3% [11]. The most common sites of metastasis are in the liver and peritoneal cavity [1]. We discuss the first documented case of primary pancreatic cancer with metastasis to the trapezium and review potential presenting symptoms that healthcare providers should be aware of for further evaluation.
Introduction
Pancreatic cancer is an aggressive disease characterized by its poor response to therapy and low survival rates. In 2023, approximately 63,050 new cases were diagnosed and there were an estimated 50,550 deaths. Incidence for pancreatic cancer has gone up by about 1% each year since the late 1990s, and the death rate has increased since that time by 0.2% per year. The combined five-year survival rate for all stages is 12%, dropping at a lower rate of 3% for metastatic disease [10,11].
The most common site of pancreatic cancer metastasis is the liver, followed by lung and peritoneal metastasis [11]. Bone and adrenal secondary tumors make up 10% of pancreatic cancer metastasis [11]. Some symptoms that may be associated with skeletal metastasis are bone pain, pathological fractures, and hypercalcemia. Although rare, it is essential for healthcare practitioners to be aware of this possibility for appropriate screening, diagnosis, and management. This case study presents the first known documented case of pancreatic cancer that metastasized to any carpal bone and specifically the trapezium.
Case presentation
An 83-year-old female with metastatic pancreatic cancer to the lungs on chemoradiation therapy and left lower extremity deep vein thrombosis on apixaban presented to the emergency department due to left hand pain and swelling for three months. The pain was primarily at the left thumb basal joint, was initially intermittent but had progressed, and she denied any trauma to that location. For the past few days the generalized swelling of the left hand had increased and was associated with redness and warmth. Ice packs and heating pads provided no relief. For her pancreatic cancer, she was treated with gemcitabine/abraxane and two cycles of FOLFOX which she tolerated poorly. She has since been treated with 5-FU/Onivyde complicated by diarrhea and weakness.
On presentation, her vitals were hemodynamically stable and she was not febrile. On examination, she was in no distress but cachectic in appearance. Physical examination revealed left thumb carpometacarpal joint swelling with erythema and no fluctuation, and range of motion was intact. Laboratory results were remarkable for elevated erythrocyte sedimentation rate of 51 mm/hr, C-reactive protein of 6.29 mg/dL, and alkaline phosphatase of 174 IntlUnit/L. Blood cultures were negative and she had no leukocytosis or elevated amylase or lipase. Magnetic resonance imaging (MRI) of the left hand revealed metastatic disease involving the entire trapezium bone and base of the first metacarpal associated with diffuse edema of soft tissue, as depicted in figure 1.
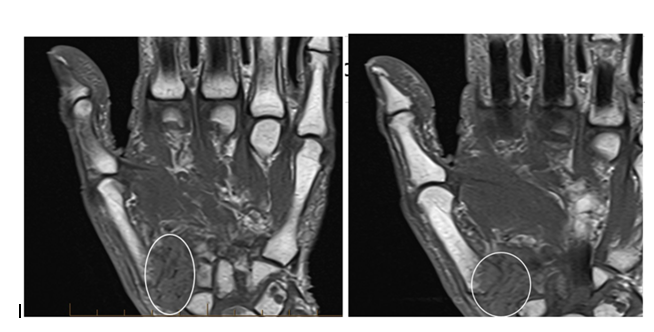
Figure 1:Metastatic involvement of entire trapezium bone and base of 1st metacarpal associated with diffuse edema of soft tissue.
Due to concern for any septic arthritis, the patient underwent incision and drainage of left thumb basilar joint and sequestrectomy of dead bone with tissue sent for pathology and culture. She was found to have edematous underlying tissue and mucopurulent material. The patient was treated with as needed pain control and was started on empiric vancomycin and ceftazidime pending culture results. Surgical and fungal culture results remained negative past 48 hours. However, surgical pathology from the necrotic bone and tissue confirmed metastatic disease depicted on MRI of the left hand and revealed metastatic moderately differentiated adenocarcinoma. By immunohistochemistry, the neoplastic cells were pancytokeratin and CK7 positive, and negative for CK20, CDX2, and TTF1. With these findings, the patient was made aware to follow up very closely with her Oncologist and given her immunocompromised state, she was discharged on ceftazidime 2g intravenous daily for six weeks.
Discussion
The common metastatic locations for pancreatic cancer are the liver, lung, and peritoneal cavity. Bone involvement from pancreatic cancer is far less likely [1]. Both osteolytic and osteoblastic lesions from osseous pancreatic metastases have been described in literature. However, our case is the first documented trapezium bone metastasis from pancreatic cancer. Prior to reviewing the current literature on the relation between pancreatic metastases and carpal hand bones, it is necessary to review the prevalence and pathogenesis of skeletal metastasis.
In a retrospective chart review study, 323 patients with pancreatic cancer were followed. The study found that seven out of 323 patients, 2.2%, developed skeletal metastasis during the course of their disease [1]. The most common site of skeletal metastasis was the vertebrae, hips and ribs were less prevalent, upper and lower extremities, skull, and face were far less common [1]. The time to development of the skeletal metastasis varied significantly with a wide range, and those with primary pancreatic cancer at the head of the pancreas had higher risk for skeletal metastasis. On the other hand, an autopsy-related study found that 5-20% of patients with pancreatic cancer can have skeletal metastases with a primary in the tail more likely to metastasize to the bone [2]. There was no documented involvement of any carpal bone during these studies, and the pathogenesis of osseous metastasis in general is not well understood.
Thus far, the pathogenesis of bone metastasis from pancreatic cancer is not well described. In general, cancer cells infiltrate and migrate to distant sites through the blood vessel wall to the extracellular space of the bone. Tumor cell adhesion is then facilitated with the aid of E- and N-cadherin [3]. Bone involvement further progresses when the physiologic remodeling process is disrupted by tumor cells. This occurs through molecular mechanisms involving cytokines such as interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF), and communication between osteoclasts, osteocytes, and osteoblasts [3].
Through literature review, there has been no documented case of pancreatic cancer with metastasis to the trapezium or any carpal bone. Two cases were found that documented involvement of the humeral bone and the clavicle. A 77-year-old female had presented due to severe tenderness at the right proximal humerus with reduced shoulder motion [5]. Further work up revealed elevated CA-19 and CEA, X-ray of the right humerus found lytic lesions with metastatic lesions. A computed tomography (CT) of the abdomen and pelvis showed a necrotic mass in the tail of the pancreas with metastasis to the left adrenal gland and liver. A tissue sample was taken from the right humerus which found metastatic Aden squamous carcinoma with mucoepidermoid morphology of pancreatic origin [5]. A prophylactic intramedullary humeral nail was placed due to fracture risk and the patient elected for conservative and symptomatic management. Most literature shows that patients who develop osseous metastasis already have concomitant visceral metastases.
The other case presented a 46-year-old female with pancreatic adenocarcinoma and subsequent Whipple procedure with six cycles of Gemcitabine, who presented with right clavicle pain two years after her procedure [6]. CT imaging showed increased sclerosis of the medial right clavicular head with a moth-eaten appearance of the cortex and medullary space. A fine needle biopsy of the right clavicle confirmed metastatic pancreatic cancer. She was started on Zoledronic Acid and completed a palliative course of radiation therapy for 2 weeks to the affected clavicle. However her course was complicated by newly developed pain in the left hip with imaging showing progression of metastatic bony disease with new lesions in the left sacrum. This presented as a unique case since no visceral metastasis was found.
Malignancy involving metastasis to the trapezium was found in three cases documented in literature. The first case involved a 62-year-old male with pain and massive swelling of the right carpometacarpal (CMC) joint of the thumb. Imaging revealed osteolytic lesions in the trapezium with resorption of almost complete resolution and a needle biopsy confirmed adenocarcinoma [7]. A PET scan and endoscopy revealed advanced gastric adenocarcinoma with no other distant metastases besides the trapezium. He underwent systemic chemoradiotherapy with eventual resection of the trapezium mass and hand reconstruction. Another case described a 70-year-old with a prior history of prostate cancer who had pain at the base of the right thumb. Work up including imaging and biopsy revealed primary non-small cell lung carcinoma (NSCLC) with trapezial metastasis [8]. Although similar, the last case presented a female in her mid-40s with known NSCLC who complained of pain at the base of her right thumb with imaging revealing trapezial involvement [9]. She underwent a trapezial excision with capsular interposition and pathology confirmed metastatic NSCLC.
Our case is the first documented in literature of trapezial metastasis from pancreatic cancer. Further information on possible screening and appropriate therapy, whether chemoradiotherapy or surgical intervention, is required. Possible skeletal survey has been considered with roentgenograms, CT, MRI, and PET scans to detect for any metastasis [1]. In those with asymptomatic skeletal metastasis, early detection could be done through serial C-telopeptide measurement [1]. However, further research into who and when to screen is required. In those with progressive carpal hand pain and risks of malignancy, we recommend further workup with imaging and biopsy to determine possible pathology.
Conclusion
The incidence of bone metastasis in primary pancreatic cancer is rare and unknown overall. Healthcare providers should be aware of these possible sites of metastasis in order to provide adequate screening, treatment, and management. This case study presented the first documented case of metastasis to the trapezium. We included relevant labs, imaging, and clinical findings and related these to other cases of pancreatic cancer with skeletal metastasis.
References
1. Borad M, Saadati H, Lakshmipathy A. Skeletal metastases in pancreatic cancer: a retrospective study and review of the literature.2009.
2. Blastik M, Plavecz E, Zalatnai A. Pancreatic carcinomas in a 60-year, institute-based autopsy material with special emphasis of metastatic pattern. 2011.
3. Vičić I, Belev B. The pathogenesis of bone metastasis in solid tumors: a review. 2021.
4. Mao C, Domenico D, Kim K, Hanson D, Howard J. Observations on the Developmental Patterns and the Consequences of Pancreatic Exocrine Adenocarcinoma: Findings of 154 Autopsies. 1995;130(2):125.
5. McCafferty J, Free M, De Villiers D, Keith P. Humeral metastases: an unusual presentation of pancreatic cancer.2022(5).
6. Saif M, Galanina N, Ravage-Mass L. Bone Metastasis as the Only Metastatic Site in a Patient with Pancreatic Cancer following Distal Pancreatectomy. 2010.
7. Okamoto M, Yamazaki H, Yoshimura Y, Aoki K, Tanaka A, Kato H. Massive trapezial metastasis from gastric adenocarcinoma resected and reconstructed with a vascularized scapular bone graft: A case report. 2017;96(50): e9294.
8. Song Y, Yao J. Trapezial metastasis as the first indication of primary non–small cell carcinoma of the lung. 2012;37(6):1242–4.
9. Gaston R, Lourie G, Scott C. Isolated metastatic lesion of the trapezium.2008;37(8):E144–5.
10. Siegel R, Miller K, Wagle N, Jemal A. Cancer statistics, 2023;73(1):17–48.
11. Pereira A, Chio I. Metastasis in Pancreatic Ductal Adenocarcinoma: Current Standing and Methodologies.. 2019;11(1):6.
Received: June 3, 2024;
Accepted: June 13, 2024;
Published: June 17, 2024.
To cite this article : Talwinder Nagi, Raksha Sharma, Elisheva Knopf, Warren Brenner. Rare Case of Pancreatic Cancer with Metastasis to the Trapezium. British Journal of Cancer Research. 2024; 7(2): 716- 717. doi: 10.31488/bjcr.196.
© The Author(s) 2024. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).